INTRODUCTION
In “A new approach to healing headaches: 1 Bioenergetic basis” I presented experimental evidence of acute cellular energy deficit involved in headaches. Simply put, whenever the brain is critically low on energy it sends a warning in the form of a pain sensation: “Whatever you are doing, it is damaging!”
But what causes this bioenergetic deficit? Is there a common cause between tension-type headaches and chronic migraine? In this article I will explore deeper insights into the origin of pain in the subjective experience of headaches. Then I will try to connect that subjective experience to the bioenergetic nature, the biology of headaches. This will allow us to search for ways of treating primary headaches.
EMOTIONAL ROOTS OF HEADACHES
It takes only a moment of recollection to realise that practically all of us have had headaches at some point in our life. With exception of the times when our headache was due to obvious reasons (secondary headache after a car accident, hangover, flu, etc), headaches commonly occur when something is out of balance: getting really tired after a long day in the office, a conflict in the family, failing an exam at school. But it takes more than just a hard day to have a headache. There is also always a very intense negative state of being.
From my own experience:
”In my research with coMra-Therapy there was a brief moment when I became very frustrated with what I perceived as me failing to reach those who are in need of healing. Suddenly I became acutely aware of things I should have done differently in the past.
For several days I barely slept and tried to work harder and harder, but I felt that I was only sinking deeper into the feeling of utter frustration with the situation that seemed to be out of my control. Then one morning I woke with a strong headache, my neck stiff and pain seeming to spread from the neck all over my head. By midday the pain grew stronger and stronger until I could no longer sit and work at my computer.
I did a brief treatment with the Delta Laser (Universal 1) but could not say that I felt an immediate major relief. Mentally and emotionally I still felt completely drained and tired, so I proceeded to do a 20 minute relaxation/meditation exercise which I have practiced for several years now.
When I emerged from the meditation, I felt in a completely different space emotionally. I felt that my perception of the situation had shifted and I felt profoundly touched by warmth towards myself. I clearly saw that in my work, in all of the huffing and puffing, I am giving my all. I acknowledged my mistakes and also that my actions were far from perfect, but I also acknowledged that I acted to the best of my knowledge at the time. I saw that my headache was caused by self-imposed expectations that were not met. After this realisation I felt a poignant and quiet sense of peace. In a few minutes my headache dissipated completely.”
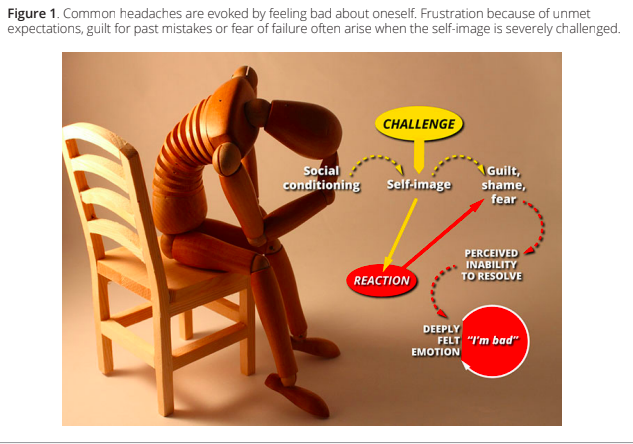
I find the most accurate description of the state of someone with a headache as given by Théun Mares [1]:
“Feeling bad about oneself, often because of a sense of guilt or a feeling of being inadequate and therefore useless”
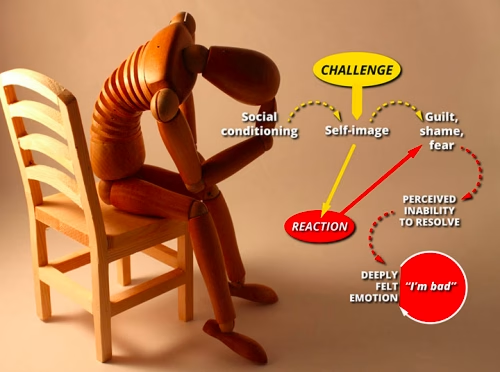
There is a huge variety of situations that may lead to intense negative emotions and so to headache. A young female may believe herself to be physically unattractive. A student may be under great pressure to succeed at school. A wife may feel being invalidated by her husband. Often the drive to overcome a challenge urges one to outperform as a student, worker, mother or provider of income, but the solution seems to be unattainable. Or, depending on the personality, a person may respond to a challenge by withdrawing and suppressing anger. Note that the person may not actually be in a position of failing at something. It is the perception of being inadequate that leads to defaulting into an intense negative state of mind (Figure 1).
FROM INTENSE EMOTION TO HEADACHE
As I described in Part 1 of this article, signal activity in the brain consumes a vast amount of energy. Sensory/ motor activity and cognition are expressed in the brain as firing of electrical signals that can be recorded with electroencephalography (EEG) (Figure 2).
Note that maintaining such electrical activity requires an energy expenditure comparable to a human leg muscle running a marathon. Moreover, the energy expenditure is directly proportional to the rate of firing of electrical signals or intensity of neuronal activity [2; 3].
From personal experience we know that intense mental activity by itself may not necessarily lead to a headache in a healthy person. Ensuing mental fatigue, feeling physically tired or even getting very bored with the task at hand may act as a safety switch. But the situation is very different once intense emotions are involved.
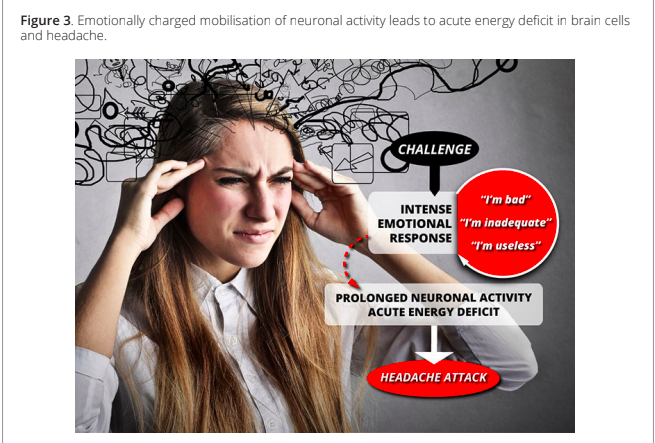
When we had to run away from a saber-toothed tiger in the not so distant past, every last energy resource in the body was spent on saving one’s life. Today it is rather our mind that is going through a “near-death” experience. When the social image of self is severely challenged and there seems to be no hope of winning, the mind locks in hyperactivity with the safety switch off.
As a result of the emotionally charged mobilisation of neuronal activity, the physical brain does not have a chance to rest and recover the dropping energy stores in cells. Muscular tension in the neck, shoulders and scalp may further aggravate the problem by mechanically impeding the blood flow and precipitating energy deficit more quickly.
As I described earlier, the deepening energy deficit can be expressed through premonitory symptoms. Feeling tired and weary is reported in 72% of attacks with warning features in migraine patients [4]. Sound or light activated sensory activity poses extra energetic demand on already depleted neurons, leading to photophobia and phonophobia, common symptoms before headache attacks. Increased blood flow or craving for food can be seen as the body trying to compensate for looming energy crises.
Finally, as stores of energy drop beyond a critical level, neurons may stop functioning completely and may even fail to maintain their internal homeostasis. During the phenomenon known as Cortical Spreading Depression neurons temporarily stop sending signals (electrical silence) and also swell because molecular pumps embedded in cell membranes do not have sufficient energy to maintain internal chemical balance. Cortical Spreading Depression is linked to the progression of visual aura when the neurons responsible for visual processing fail to function normally.
At this stage of acute pain, a headache attack is in full force (Figure 3).
CHRONIFICATION OF HEADACHES
Occasional headaches can easily be linked to feeling down and stress. But how can we explain when severe headache attacks become semi-regular and can be triggered by normally harmless events, such as eating certain foods, lack of sleep or dehydration? Does this mean that a chronic disease such as episodic migraine is a completely different disorder from occasional tension-type headaches?
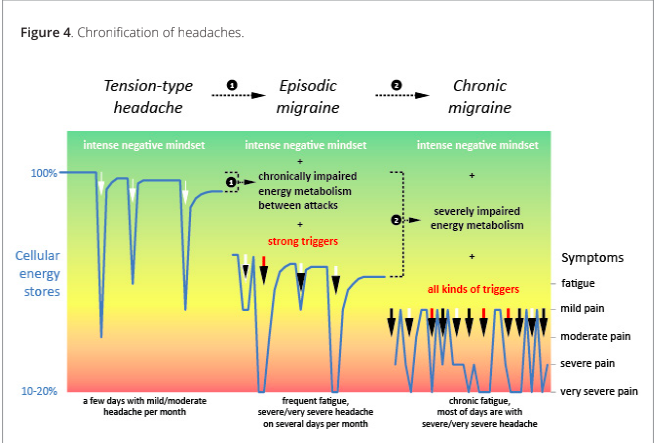
Detailed observations of many headache patients revealed that primary headaches represent one continuum rather than completely separate entities [5]. Clinically it has been observed that patients with tension-type headaches (mostly mild to moderate pain) can experience them over time transforming into episodic migraine (semi-regular attacks of severe pain with nausea, vomiting). And 3 to 14% of patients with episodic migraine can experience them transforming into chronic migraine when headaches are present on more than 15 days per month [6].
The continuum of primary headaches led to a search of a common biological process that can progressively express symptoms of different severity. Borsook et al presented a comprehensive overview of how gradual accumulation of functional and structural changes in the course of the disease leads to worsening symptoms and effects on the brain and the whole body through systemic neuronal and endocrine physiology [7].
For our discussion, the key experimental observation in chronification of headaches is that cellular energy stores are no longer recovered to normal levels between headache attacks [8]. Each attack cumulatively adds wear and tear on energetic metabolism in cells to the point when abnormal changes in mitochondria (cellular power plant) can be seen even microscopically [9]. Purely emotional/mental causes of headache become aggravated by chronically impaired energy metabolism in cells.
Once the energy metabolism in cells becomes severely damaged, attacks can be triggered by any type of disturbance, because cellular energy stores are near critical levels at all times. This severely impaired energy metabolism creates a bioenergetic deficit on its own, establishing a vicious circle (Figure 4).
DISCUSSION
I have presented a brief outline of a holistic view of the causes of primary headaches. Previously, a very large number of studies have attempted to find links between headaches and biochemical imbalances, genes, climate, socio-economic conditions, life-style and other medical conditions. But now, with this new view, several most prominent features of primary headaches appear in a new light.
Why do females have headaches more frequently than males? This fundamental difference has puzzled scientists for ages. In headaches, and especially in the most debilitating headaches such as migraine, females have the condition about twice as often as males. This trend is preserved across countries and continents [10]. But common sense allied with this new view suggests that females are more prone to headaches because they are naturally more sensitive and in tune with their feelings which, in case of intense negativity, can be expressed as a headache.
Another very well-known fact about migraine and other primary headaches is that that they tend to run in families [11]. The inheritance of migraine from parent to child has been documented since the 17th century and the disease has been described as “in essence a familial episodic disorder whose key marker is headache, with certain associated features …” [12]. First degree relatives of a person with cluster headaches have a 14-fold increase in chances of having cluster headaches [13]! And yet genetic studies have not discovered any specific headache genes for common migraine or cluster headaches.
But are genes the only things we inherit from our parents? There is also a constant subconscious learning of mindset and behaviour. A toddler may not understand in rational terms what is happening around her, but on a feeling level she can easily pick up how her mother feels when things are not going well. The child may not necessarily experience headache at the time but what is important is that a certain behavioural pattern is being established.
Obviously, primary headaches can also occur even when parents do not have the condition. If the headache is extremely debilitating, often its origins can be traced to a traumatic experience in childhood or later in life, if the event had a very strong and lasting impact, such as physical abuse, going through puberty, divorce, etc.
In the next article I will discuss the healing of headaches.
ACKNOWLEDGEMENTS
This article has been inspired by ideas of late Théun Mares. A lot of headache sufferers, doctors and healers openly shared with me their observations and helped me in the development of this article. Thank you!
REFERENCES
- Mares, T. Health and holism in the 21st century. unpublished.
- Hyder, F., et al. 2013. Cortical energy demands of signaling and nonsignaling components in brain are conserved across mammalian species and activity levels. Proceedings of the National Academy of Sciences no. 110 (9):3549-3554. doi: 10.1073/pnas.1214912110.
- Attwell, D., et al. 2001. An energy budget for signaling in the grey matter of the brain. Journal of Cerebral Blood Flow & Metabolism no. 21 (10):1133-1145. doi: 10.1097/00004647-200110000-00001.
- Giffin, N., et al. 2003. Premonitory symptoms in migraine An electronic diary study. Neurology no. 60 (6):935-940. doi: 10.1212/01.WNL.0000052998.58526.A9.
- Cady, R., et al. 2002. Primary Headaches: A Convergence Hypothesis. Headache: The Journal of Head and Face Pain no. 42 (3):204-216. doi: 10.1046/j.1526-4610.2002.02053.x.
- Bigal, M., et al. 2011. Migraine Chronification. Current Neurology and Neuroscience Reports no. 11 (2):139- 148. doi: 10.1007/s11910-010-0175-6.
- Borsook, D., et al. 2012. Understanding Migraine through the Lens of Maladaptive Stress Responses: A Model Disease of Allostatic Load. Neuron no. 73 (2):219-234. doi: 10.1016/j.neuron.2012.01.001.
- Lodi, R., et al. 2001. Deficient energy metabolism is associated with low free magnesium in the brains of patients with migraine and cluster headache. Brain Research Bulletin no. 54 (4):437-441. doi: 10.1016/S0361-9230(01)00440-3.
- Sparaco, M., et al. 2006. Mitochondrial dysfunction and migraine: evidence and hypotheses. Cephalalgia no. 26 (4):361-372. doi: 10.1111/j.1468-2982.2005.01059.x.
- Stovner, L.J., et al. 2007. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia no. 27 (3):193-210. doi: 10.1111/j.1468-2982.2007.01288.x.
- van den Maagdenberg, A.M., et al. 2007. Migraine: gene mutations and functional consequences. Current Opinion in Neurology no. 20 (3):299-305 10.1097/WCO.0b013e3281338d1f.
doi: 10.1097/WCO.0b013e3281338d1f.
- Goadsby, P.J. 2012. Pathophysiology of migraine. Annals of Indian Academy of Neurology no. 15 (Suppl 1):S15-22. doi: 10.4103/0972-2327.99993.
- Russell, M.B.r., et al. 1995. Familial occurrence of cluster headache. Journal of Neurology, Neurosurgery & Psychiatry no. 58 (3):341-343. doi: 10.1136/jnnp.58.3.341.
Acknowledgements: This article has been inspired by ideas shared with me by Théun Mares. Development of the article has been done with my friends at Radiant Life Technologies.
----
License: © Copyright 2014, Surazakov. This article is distributed under the Creative Commons license, which permits unrestricted use and redistribution provided that the original author and source are credited.